

A new report released by the Global Network of People Living with HIV (GNP+), the International Community of Women Living with HIV (ICW), and other local network partners, calls for dignity and rights in family planning programmes for women living with HIV in Cameroon, Nigeria and Zambia. that calls for discrimination-free family planning services for women living with HIV. The study examined the experiences of women living with HIV in accessing family planning services.
Type: Reports and briefings
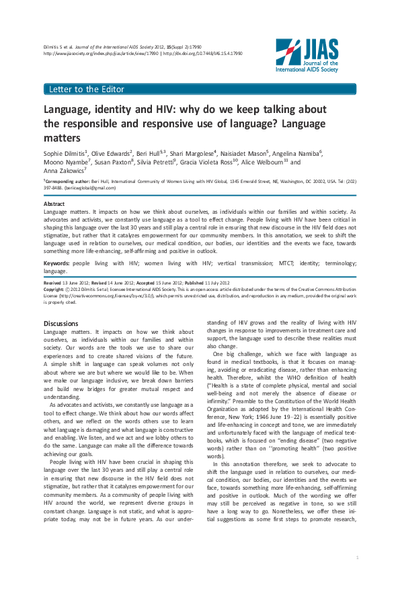
Positive Health, Dignity and Prevention. Findings and recommendations from a study led by and among people living with HIV in Swaziland 2012
At 26% Swaziland’s HIV prevalence is the highest among adults in the world (UNAIDS, 2010). An estimated 210,000 people of all ages are living with HIV in Swaziland. The increasing availability of HIV treatment has enabled people living with HIV (PLHIV) to live longer, healthier lives, and to engage in issues that directly impact on their lives and those of their partners, families and communities. In 2011, the Dutch Postcode Lottery funded a proposal submitted by STOP AIDS NOW! and the MaxART consortium, whose primary objective was to maximize access to antiretroviral treatment (ART) in Swaziland. The scale up in access to, and uptake of, HIV testing and treatment has set the stage for an implementation study to put into practice the exciting new evidence that HIV treatment can also serve as a means of prevention. One of the components of the project was the documentation of the needs and realities of PLHIV in Swaziland, in the context of the national scale-up of access to ART. This helped to continuously improve and develop evidence informed activities.
To this end, MaxART partner organization Swaziland National Network of People Living with HIV and AIDS (SWANNEPHA), with support from the Global Network of People Living with HIV (GNP+), conducted a cross-sectional survey among PLHIV to document their experiences in relation to Positive Health, Dignity and Prevention (PHDP) which promotes holistic health and wellness, including human rights, legal protections, policy environment free of stigma and discrimination for PLHIV as well as access to HIV treatment, care and support services and by doing so contributes to the health and wellbeing of their partners, families and communities. A total of 919 people were reached from the four regions of Swaziland with the support of expert clients who are also people living with HIV.
This report presents the findings of the PHDP survey and it describes the experiences of PLHIV in the context of the national scale up of HIV testing, care and treatment with highlights of the important linkages between prevention, treatment, care, support and human rights. This will go a long way to inform evidence based PHDP programming. The findings of the study were analyzed in relation to the following PHDP components: empowerment, gender equality, health promotion and access, human rights, prevention of new infections, sexual and reproductive health and rights, and social and economic support.
In mid-January 2015, women living with HIV came together with the World Health Organisation (WHO) to consult and give input to a global survey on sexual and reproductive health and human rights of women living with HIV. Dr Manjulaa Narasimhan of WHO’s Reproductive Health and Research Department led on conducting the survey, which will inform WHO as it updates its 2006 guidelines on this topic.
Summary Report of Proceedings: COUNTRY TO COUNTRY SHARING MEETING
13–14 December 2013, Nairobi, Kenya
The concept for the Framework for Dialogue was born in 2010 out of a mutually agreed desire for sustained and systematized action-oriented dialogue between faith communities/ religious leaders and networks of people living with HIV for the purpose of contributing to an effective response to HIV at country level.
The first (pilot) dialogue was held in Malawi in May 2012, with further pilots in Ethiopia and Myanmar. Following the pilots, Uganda held its first dialogue in December 2013. Kenya is one of the other countries planning to implement the process in 2014.

A summary report of the HIV Leadership through Accountability final project meeting held in Dakar, Senegal 3-5 June, 2013.
The side event “Post-2015 Development Framework…what’s in it for young people?” was held following the General Assembly 68th Session’s High Level Event on the MDGs and brought together representatives of UN Member States, UN agencies and civil society, as well as key politicians and young people living with and affected by HIV. The aim was to facilitate an open and frank discussion with young people living with and affected by HIV and representatives of key population groups giving them a voice in the global post-2015 debate and to better understand the challenges they face in accessing comprehensive HIV and sexual and reproductive health services and their needs and hopes for the future.
The event was co-organized by the African Services Committee, the Global Youth Coalition on HIV/AIDS (GYCA), the HIV Young Leaders Fund , Housing Works, ICASO, International AIDS Vaccine Initiative (IAVI), International Civil Society Support (ICSS), the International HIV/AIDS Alliance, the International Women’s Health Coalition and STOP AIDS NOW!.

The criminalisation scan in Tanzania was undertaken by the Tanzania National Council of People Living with HIV and AIDS (NACOPHA) with the objective to map and document the existence of laws, practices and policies in existence in Tanzania that have an impact on responses to HIV.
For more information on criminalisation in Africa and its countries, visit the the GNP+ criminalisation scan website
This report reviews the combined findings and recommendations of research conducted by NEPHAK using five GNP+ evidence gathering tools, trying to answer the questions how we can create a Positive Health, Dignity and Prevention (PHDP) Framework for Kenya. It explores whether the evidence contained within the five reports to describe the country’s progress towards achieving the values of PHDP and to document the existence and performance of the programmatic components (policies, services and initiatives) are ready to be integrated into a national PHDP framework, and then highlights recommendations most likely to improve the health and dignity of PLHIV in Kenya.
A thematic review was performed of the findings, conclusions and recommendations to search for any significant reference to the key PHDP themes and issues, as described by the PHDP Policy Framework. Observations were made on any topic which was not addressed in the LTA research.
The report summarises the key findings of the review, and describes the key barriers and opportunities to advance PHDP as suggested by the thematic analysis and the action steps for PHDP advocacy that can be drawn from the LTA research recommendations.
The Nigerian Network NEPWHAN used the data of the five evidence gathering tools that were implemented in the country to analyse in how far the country was working within the positive health, dignity and prevention framework. PHDP looks at people with HIV in a holistic way and within a human rights framework. You can read more about what this means here.
Why do we keep talking about the responsible and responsive use of language? Language matters
Language matters. It impacts on how we think about ourselves, as individuals within our families and within society. As advocates and activists, we constantly use language as a tool to effect change. People living with HIV have been critical in shaping this language over the last 30 years and still play a central role in ensuring that new discourse in the HIV field does not stigmatize, but rather that it catalyzes empowerment for our community members. In this annotation, we seek to shift the language used in relation to ourselves, our medical condition, our bodies, our identities and the events we face, towards something more life-enhancing, self-affirming and positive in outlook.
Keywords: people living with HIV; women living with HIV; vertical transmission; MTCT; identity; terminology; language
(Published: 11 July 2012)
Citation: Dilmitis S et al. Journal of the International AIDS Society 2012, 15 (Suppl 2):17990
http://www.jiasociety.org/index.php/jias/article/view/17990 | http://dx.doi.org/10.7448/IAS.15.4.17990
For more information on The People living with HIV Stigma index, visit the the GNP+ PLHIV stigma index website
This study was conducted by the National Association of People living with with HIV & AIDS as part of the HIV leadership through accountability programme. The aim of the study was to map and document existing laws, and policies that impact on responses to HIV in South Africa.
The criminalisation scan documents protective as well as punitive laws and policies as they relate to people living with HIV and key populations at higher risk of HIV infection. The study found that while post apartheid South Africa has one of the most extensive bills of rights in the world, many of the protective laws and policies are not adequately promoted and enforced, with the result that many people suffer dicrimination and abuse.
This is a report on a study conducted with Lesbian, Gay, Bisexual, Transgender and Intersex (LGBTI) people to explore their Sexual and Reproductive Health and Rights experiences and needs. The research exercise involved HIV positive LGBTI people and LGBTI NGOs in Kwa-Thema in Springs, Gauteng, South Africa. The main objective of the research was to collect data on sexual and reproductive health needs and experiences of LGBTI community, especially among people who are living with HIV.
This study was carried out by the National Network of Positive Women Ethiopia (NNPWE) in collaboration with GNP+ and NEP+. The study is an expansion of an earlier study focusing on the Adama and Addis Abeba regions. The study concludes that while policies are well defined, there are large gaps due to poor infrastructure and limited resources. Knowledge has increased but there remains large difference betwen urban and rural settings.
GNP+ at ICASA 2011 held a liaison meeting for focal points from networks of people liivng with HIV involved in the HIV Leadership through accountability programme. The meeting included 18 people of 10 different networks.
Main issues discussed were:
- Update of programmes in the different countries;
- Collaboration around LIVING 2012.
The National Association of People Living with HIV and AIDS (NAPWA) would also like to thank the Global Network of People Living with HIV (GNP+) and the United Kingdom’s Department for International Development (DFID) Governance and Transparency Fund (GTF). Their financial and technical support made this study possible.
The mission statements and goals of the participating organisations covered a wide range of activities aimed at addressing the HIV epidemic. These included, improving the lifestyles of people, monitoring and evaluating programmes, providing technical support to health service providers, supporting government, conducting testing campaigns, encouraging home based care and support, developing Integrated Development Programmes (IDPs) and LGBTI services, enhancing delivery and empowering sex workers. Some participants did not provide information about their mission statements.
This report was produced as part of HIV Leadership through Accountability programme, which ran for five years, from 2009 to 2013
It was spearheaded Global Network of People Living with HIV (GNP+) and the World AIDS Campaign (WAC), and funded by the Department for International Development (DfID), to create evidence-based campaigning, advocacy and lobbying for and by people living with HIV. Research was carried out to inform and strengthen national, regional and international advocacy, and was implemented with a bottom-up approach, informed by community responses, and strengthened by South-South collaboration.
The countries where the programme was implemented were: Cameroon, Ethiopia, Kenya, Malawi, Moldova, Nigeria, Senegal, South Africa, Tanzania and Zambia.
More information and background materials can be found at http://www.hivleadership.org/ which is the archive site for the programme
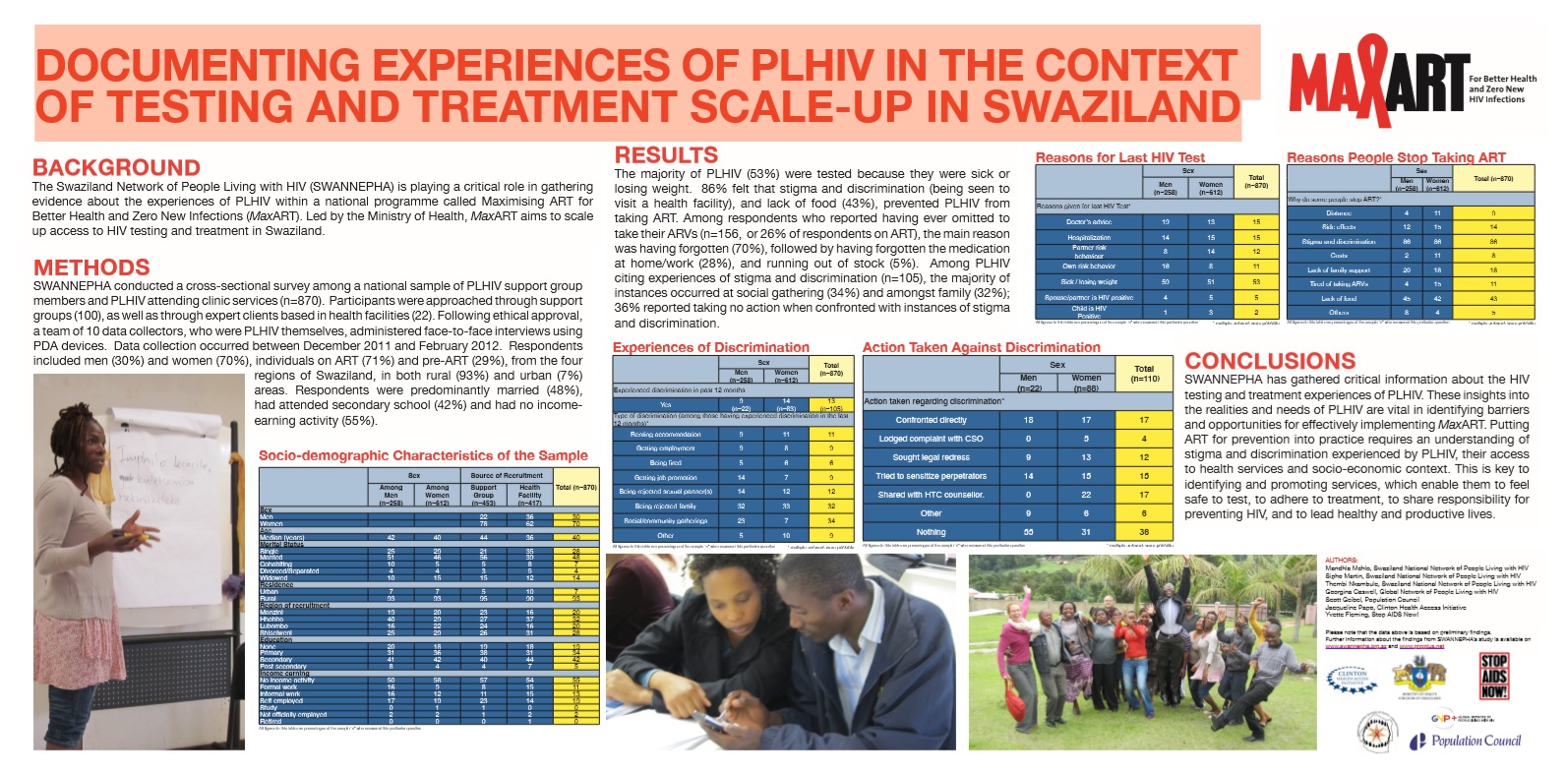
HIV is a major obstacle to employment security. People living with HIV may be unable to find or maintain employment as a result of ill health. However, evidence from the People Living with HIV Stigma Index (PLHIV Stigma Index) reveals that HIV-related stigma and discrimination are as frequently or more frequently a cause of unemployment/denial of work opportunity as ill health in many national settings.
This evidence brief has been prepared by the Global Network of People Living with HIV (GNP+), and was funded by the ILO Programme on HIV/AIDS and the World of Work (ILO/AIDS). It includes PLHIV Stigma Index findings from nine countries in four regions: Kenya, Nigeria and Zambia (sub-Saharan Africa), Estonia and Poland (Eastern Europe), Malaysia and the Philippines (Asia-Pacific,) and Argentina and Mexico (South America). PLHIV Stigma Index data clearly shows that HIV-related stigma and discrimination directly impede access to work by people living with HIV by:
- obstructing entry to the labour market
- changing the type of work individuals are allowed to perform
- preventing promotion to more senior positions
- triggering people being fired from their jobs
- impeding access to adult education and training
A poster presentation with a summary of its findings are available here.